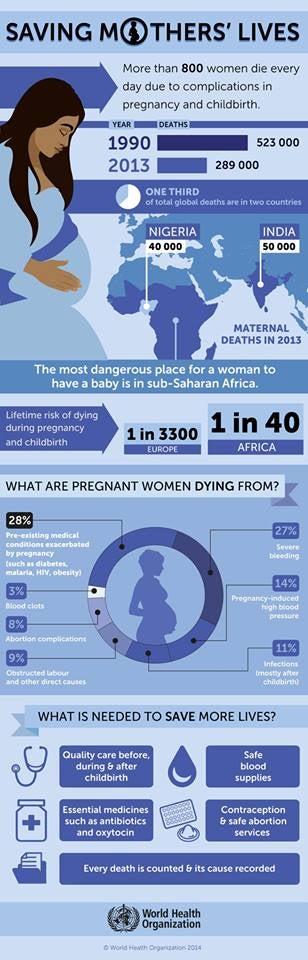
Whatever you've decided will fill your current 24 hours, 800 women will die within that same hour from pregnancy or childbirth complications; that's 33 women dying every hour from conditions that could be prevented.
The absence of a global outcry at this aspect of maternal health or reproductive health is deafening - perhaps it is indeed one of the hazards of pregnancy but what should irk you as a fellow human being is the fact that 289,000 maternal deaths occurred in 2013, in this age of advanced technology, when it is almost the norm to conduct surgeries via the internet.
The status of maternal mortality in the 15 Pacific island countries including Papua New Guinea (PNG) is a mixed bag - most Polynesian countries will achieve MDG5a (eliminate maternal mortality) while most Melanesian countries won't, though compared to 1990, reported skilled birth attendant rates have increased in all countries except Federated States of Micronesia (FSM), PNG and Vanuatu.
The Pacific regional review in 2013 of how countries had performed in the implementation of the International Conference on Population and Development's (ICPD) Programme of Action (PoA) reports that while countries have contributed in various ways towards the improved delivery of sexual and reproductive health (SRH) services, no Pacific country had specifically allocated SRH in their annual national budgets and very few had opted out of donor partner support for the purchase of their contraceptives.
Contraceptive prevalence rate (CPR) remained below 50 per cent, the review found and while most remained static, only the Cook Islands, FSM, Fiji and the Republic of the Marshall Islands (RMI) would occasionally record a high of 40 per cent.
If countries were to meet unmet needs (women who desire to delay or stop childbearing but cannot access contraceptives for various reasons), this could reduce the maternal mortality ratio between 25 to 40 per cent. In the Pacific, unmet need vary from 1 per cent to 40 per cent and in most countries, unmet need rates are similar in both rural and urban areas.
"Some Pacific island nations do not record maternal mortality anymore while some are continuing to work towards its elimination, but we should join our efforts to ensure that no woman dies at the moment of delivery in the Pacific," Dr Laurent Zessler, UNFPA Pacific Director and Representative said.
During the recent United Nations Population Fund (UNFPA) Pacific Sub-Regional Office-organised regional meeting of permanent secretaries of health, the need for countries to treat reproductive health issues as development issues was reiterated. This would inevitably require introspective of (our) governance philosophies.
Maternal mortality is a personal issue as it is reflective of both our attitudes as individuals and collectively as societies towards girls and women, who aren't usually accepted as individuals first and foremost, with inalienable human rights, before gender or any other cultural or faith-based considerations.
Maternal mortality is a development issue because it is reflective of how much the duty-bearers, our governments, are meeting their obligation in terms of health services for right-holders, we the citizens.
It is a development issue because realities that continue to neglect the good health and/or environment that does not enable girls and women to have autonomy over their own bodies eventually manifests in a country's general progress - neglect the good reproductive health of half the populace and the country deprives itself of much-needed human resources and half its productivity potential.
Maternal mortality is a development issue because United Nations (UN) member states are signatories to the 56th Session of the United Nations Commission on the Status of Women in 2012 which adopted a resolution on "eliminating maternal mortality and morbidity through the empowerment of women..." and because it is one of the main indicators of the Millennium Development Goal 5, monitored by the UN and reported on regularly.